Introduction: The Next Phase of Peer Support Development
Peer support, a cornerstone of recovery-oriented behavioral healthcare, is a rapidly expanding service model nationally. Delivered by individuals with lived experience of mental health challenges, substance use, trauma, or disability, peer supporters use shared experience, mutuality, and hope to provide relational support to others undergoing similar challenges. First introduced as a service model in 1991, peer support became Medicaid-reimbursable in 2007, and programs in 48 states and the District of Columbia offer reimbursement for these services currently. Forty-nine states have peer certification processes, and over 100,000 people have been trained nationwide.
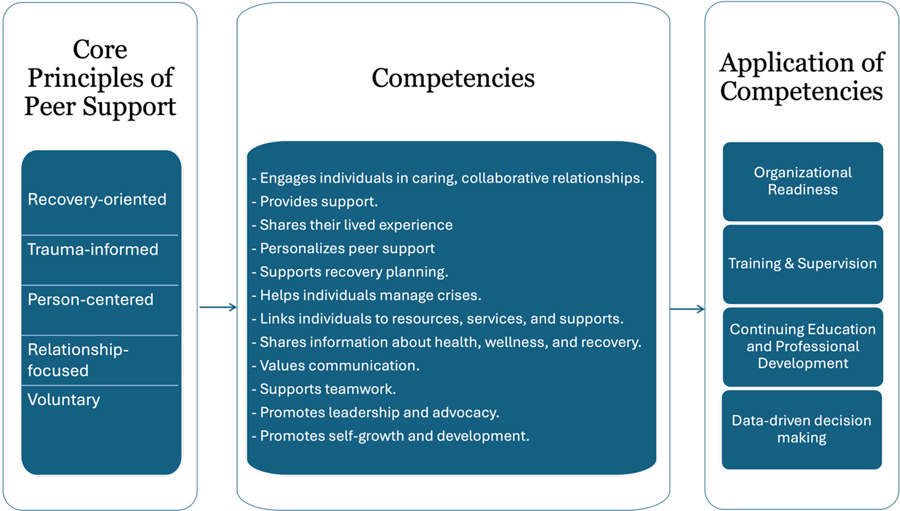
Figure 1: Application of core competencies of peer support
As the peer workforce continues to grow, it is important to build the infrastructure needed to support it. Because peer support is delivered in many different settings and ways, questions such as the following have emerged:
- How can organizations make sure peer support stays true to its core values?
- How can systems measure the impact of peer support while maintaining its relationship-based nature?
- How can we scale the workforce to meet client needs without losing the value of lived experience?
Addressing these questions requires moving toward the next phase of workforce development: developing a peer-informed fidelity measure to assess whether peer support is being delivered as intended. National efforts led by the Substance Abuse and Mental Health Services Administration (SAMHSA) helped identify core competencies of peer support. These competencies guide training, certification, and role clarity while strengthening the recognition of peer work and maintaining its recovery-focused values.
Core Competencies as a Foundation for Peer Workforce Development
SAMHSA’s core competencies of peer support (Figure 1) are grounded in the following values:
- Recovery-oriented
- Trauma-informed
- Person-centered
- Relationship-focused
- Voluntary
Competency frameworks can help clarify peer roles, inform training programs, and support the development of certification standards across states. They can provide a shared language that helps organizations understand what peer support is, and what it is not, providing clarity around the peer support role.
While these competencies define what peer support should look like, they do not necessarily provide tools for assessing whether those practices are being implemented in real-world settings. This gap has important implications for both workforce sustainability and research.
Why Measurement Matters for Peer Support
The peer movement began as a response to traditional systems of care and was grounded in values such as empowerment, mutuality, and social justice. These principles are not always captured by traditional clinical measures. Behavioral health systems often rely on data to inform funding decisions, program development, and service evaluation. Many studies of peer services focus on broad outcomes such as hospitalization rates, symptom reduction, or service utilization. While these outcomes are important, they do not necessarily make clear what exactly is being evaluated or the ways in which peer support was delivered. Because of this, researchers and policymakers have struggled to determine when peer support is being delivered with fidelity to its core principles.
This creates what some describe as a “black box” problem for peer support research. If we cannot measure how peer support is delivered in practice, it becomes difficult to evaluate what makes it effective, or to ensure that programs maintain the integrity of the peer role as they grow.
To address this gap, researchers at the Yale Program for Recovery and Community Health have begun work to develop a competency-based fidelity measurement tool that focuses on assessing the defining elements of peer support and how they are delivered in research and practice. Below we discuss four ways this type of tool could benefit behavioral health organizations.
1. Assesses Organizational Readiness
One promising approach to using a competency framework is as a tool to assess organizational readiness and guide efforts to prepare the organizational culture for the integration of peer support workers. At this stage, organizations can review whether their policies, practices, and culture align with recovery-oriented peer values before introducing peer roles.
2. Guides Training and Supervision
Competency frameworks are currently used to guide certification requirements but can also serve as a valuable tool for training and supervision within organizations that employ peer workers. When used thoughtfully, competency-based approaches can help ensure that peer workers receive professional support while preserving the relational and recovery-oriented foundations of peer work.
Training programs that align with peer support competencies provide a structured way to introduce the values and practice of peer work. Instead of focusing only on job tasks, competency-based training highlights the values and relationship skills that make peer support different from traditional clinical roles. These include practices such as using lived experience intentionally, fostering mutuality, promoting hope, supporting self-determination, and helping individuals navigate complex behavioral health and social service systems.
Supervision represents another critical area where competency frameworks can strengthen peer workforce infrastructure. Traditional clinical supervision models are not always well suited to the unique nature of peer work. Peer support emphasizes shared experience, empowerment, and mutual learning, principles that may be misunderstood if supervision is grounded exclusively in hierarchical clinical models.
Competency-based supervision offers a more supportive alternative. Supervisors can use competency frameworks to guide reflective discussions about how peer workers are applying the principles of peer support in their daily practice. Conversations may focus on how peer workers use lived experience appropriately, maintain ethical boundaries while preserving mutuality, or support individuals in identifying and pursuing personal meaningful recovery goals. Overall, competency-based training and supervision help ensure that peer workforce development remains aligned with the foundational values of recovery, empowerment, and lived experience leadership. By grounding training and supervision in these principles, organizations can support peer workers while strengthening the integrity of peer support within behavioral health systems.
3. Structures Continuing Education and Professional Development Opportunities
As peer workers gain experience, organizations can use competencies to identify areas for skill development, such as facilitating peer groups, supporting individuals from diverse cultural backgrounds, practicing trauma-informed engagement, or participating in program evaluation and quality improvement efforts. In this way, competencies help create clearer professional development pathways for peer workers while aligning continuing education with the changing needs of the workforce.
4. Increases Data-Driven Decision-Making
As peer support programs expand across behavioral health systems, organizations are increasingly asked to demonstrate the effectiveness and impact of peer services. Competency-based fidelity measurement is the first step toward making data-driven decisions. Instead of immediately focusing on outcomes, fidelity approaches examine whether peer support services are being delivered in ways that reflect the core principles and practices that define peer work. By assessing whether these elements are present in service delivery, organizations can better understand how peer support is being implemented and identify areas for improvement. Then, when going on to measure outcomes, organizations better understand the extent to which peer support programming was implemented as intended.
Fidelity data can help organizations strengthen workforce development strategies. For example, if assessments show challenges related to role clarity, boundary navigation, or integration within interdisciplinary teams, organizations can respond by refining training programs or supervision models. In this way, fidelity measurement supports continuous quality improvement rather than simply monitoring performance.
Competency-based fidelity measures can also help demonstrate the impact of peer support to policymakers, funders, and health systems. As behavioral health systems increasingly rely on data to guide funding and program decisions, having tools that capture the unique elements of peer support can help demonstrate the value of lived experience-based services.
When implemented thoughtfully, fidelity measurement can strengthen the peer workforce by giving organizations useful insights while protecting the relational and recovery-oriented principles that make peer support unique.
Conclusion: Looking Ahead- Building a Balanced Infrastructure for Peer Support
Competency frameworks provide important guidance for training, supervision, and quality improvement. Measurement tools, including emerging competency-based fidelity measures that build on previous work in the field, can help ensure that peer support is delivered in ways that reflect its core principles.
At the same time, these tools must be implemented carefully. If competencies and measurement strategies are applied without attention to mutuality, equity, and lived experience leadership, peer support could become a checklist of tasks instead of a relationship-based practice. Tools must go beyond a simple checklist of “did they do the step?” to also measure the skills, accuracy, and approach used by peers to ensure the service is delivered in a way that supports the intended outcomes. Any peer support fidelity measure needs to consider both the what of peer support (e.g., tasks and activities) as well as the how (e.g., relational aspects).
The most promising path forward is a community-engaged approach: developing competency and measurement tools through partnering with peer support and lived experience leaders across the country. As the workforce expands, evaluation efforts must keep pace. The sustainability of this emerging workforce depends upon it.





For more information, contact Megan Evans, PhD at megan.evans@yale.edu.
Megan Evans, PhD, is an Associate Research Scientist at the Yale School of Medicine, Department of Psychiatry, Yale Program for Recovery and Community Health (PRCH), and can be reached at Megan.evans@yale.edu. Kristine Irizarry, MBA, is a Program Manager at the Yale School of Medicine, Department of Psychiatry, Yale Program for Recovery and Community Health (PRCH), and can be reached at Kristine.irizarry@yale.edu. Sai Snigdha Talluri, PhD, CRC, LPC, is a Postdoctoral Associate at the Yale School of Medicine, Department of Psychiatry, Yale Program for Recovery and Community Health (PRCH), and can be reached at saisnigdha.talluri@yale.edu. Graziela Reis, MPH, BS, is a Research Coordinator at the Yale School of Medicine, Department of Psychiatry, Yale Program for Recovery and Community Health (PRCH), and can be reached at Graziela.reis@yale.edu. Chyrell D. Bellamy, PhD, MSW, is a Professor and Director of the Yale Program for Recovery and Community Health (PRCH) at the Yale School of Medicine, Department of Psychiatry, and can be reached at Chyrell.bellamy@yale.edu.
References
Bringing Recovery Supports To Scale. (n.d.). https://www.samhsa.gov/sites/default/files/core-competencies-peer-workers-behavioral-health-services.pdf
Chinman, M., McCarthy, S., Mitchell-Miland, C., Daniels, K., Youk, A., & Edelen, M. (2016). Early stages of development of a peer specialist fidelity measure. Psychiatric Rehabilitation Journal, 39(3), 256–265. https://doi.org/10.1037/prj0000209
Davidson, L., Bellamy, C., Guy, K., & Miller, R. (2013). Peer support among persons with severe mental illnesses: A review of evidence and experience. World Psychiatry, 11(2), 123–128. https://doi.org/10.1016/j.wpsyc.2012.05.009
Evans, M., Cuddeback, G. S., Golin, C., Muessig, K., Bellamy, C., Costa, M., O’Connell, M., & Fisher, E. B. (2024). Diverse elements comprising studies of peer support complicate evidence synthesis. Journal of Mental Health, 1–15. https://doi.org/10.1080/09638237.2024.2332798
Larry Davidson, P., Chyrell Bellamy, M. S. W., Mathew Chinman, P., Marianne Farkas, S., Laysha Ostrow, P., Judith A. Cook, P., Jessica A. Jonikas, M. A., Rosenthal, H., Bergeson, S., Allen S. Daniels, E., & Mark Salzer, P. (2018). Revisiting the Rationale and Evidence for Peer Support. Psychiatric Times, 35(6). https://www.psychiatrictimes.com/view/revisiting-rationale-and-evidence-peer-support
Yale Program for Recovery and Community Health. (2024). Yale Program for Recovery and Community Health. https://medicine.yale.edu/psychiatry/prch/


